Physiological Mechanisms
When a placebo is administered to a patient and the patient experiences an effect, either positive or negative, physiological changes have been recorded in accordance with that outcome. What is important to note is that the type of physiological response exhibited by the patient differs depending on the condition being treated. Below we will discuss the physiological effects of placebo analgesia and dopamine release.
When a placebo is administered to a patient and the patient experiences an effect, either positive or negative, physiological changes have been recorded in accordance with that outcome. What is important to note is that the type of physiological response exhibited by the patient differs depending on the condition being treated. Below we will discuss the physiological effects of placebo analgesia and dopamine release.
Placebo Analgesia
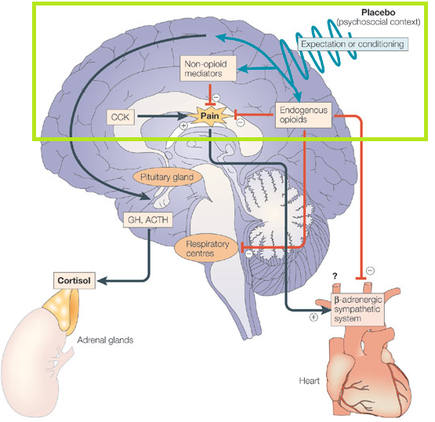
Several mechanisms have been proposed surrounding how placebos given for pain can effect signalling patterns in the body, particularly in the brain. Many of these mechanisms are discussed in an article by Benedetti et al. One mechanism these authors discuss is that when a placebo is given for pain it can involve the recruitment and activation of the body's endogenous opioids or endorphins. Endorphins are "neurotransmitters that can interact with opiate receptors in the brain to reduce our perception of pain". One study that helped to prove that endorphins can be released upon administration of placebo was completed by Levine et al in 1978. The study looked at patients who had just undergone extraction of impacted molars. All patients were given diapzepam, nitric oxide, and mepivacaine. Then, at 3 hours post surgery, patients were randomly given either naloxone, an opiate antagonist, a placebo, or morphine (note that people given morphine were later excluded). At 4 hours post surgery the patients were again randomly given any of the above three options. The results of this study were particularly interesting because when placebo was given first, and if patients reported an improvement in pain, when naloxone was given, an increase in pain was experienced. If the patients who were given placebo first did not respond to the placebo, the addition of naloxone did not change patients' pain. This supports the hypothesis that endogenous opioids may be involved in the placebo analgesia response. To read the whole study please visit the additional resources page on this website to see the full referencing information.
The review article by Benedetti et al also mentions other mechanisms proposed regarding the physiology of placebo analgesia. They discuss mechanisms involving non-opioid mediators and cholecystokinin. In terms of non-opioid mediators, a study by Amanzio and Benedetti in 1999 showed that patients who underwent conditioning (see our theories page for more information on conditioning) with the drug Ketorolac experienced a placebo response that was non responsive to naloxone, meaning that the addition of naloxone after giving a placebo that produced a response, did not cause more pain in the patient. Therefore, other pathways besides the endogenous opioid pathway mentioned by Levine et al must be present in effects experienced through administration of placebo analgesia. Cholecystokinin (CCK) has also been proposed to be involved in the analgesia response experienced by patients given placebo. CCK exhibits the opposite action of opioids. In one study, when proglumide, a drug which blocks CCK was given, the relief of pain experienced by placebo was enhanced, thereby indicating CCK may also have a role in analgesia experienced through adminstration of a placebo. See the green box in the diagram above for more on these mechanisms.
Several mechanisms have been proposed surrounding how placebos given for pain can effect signalling patterns in the body, particularly in the brain. Many of these mechanisms are discussed in an article by Benedetti et al. One mechanism these authors discuss is that when a placebo is given for pain it can involve the recruitment and activation of the body's endogenous opioids or endorphins. Endorphins are "neurotransmitters that can interact with opiate receptors in the brain to reduce our perception of pain". One study that helped to prove that endorphins can be released upon administration of placebo was completed by Levine et al in 1978. The study looked at patients who had just undergone extraction of impacted molars. All patients were given diapzepam, nitric oxide, and mepivacaine. Then, at 3 hours post surgery, patients were randomly given either naloxone, an opiate antagonist, a placebo, or morphine (note that people given morphine were later excluded). At 4 hours post surgery the patients were again randomly given any of the above three options. The results of this study were particularly interesting because when placebo was given first, and if patients reported an improvement in pain, when naloxone was given, an increase in pain was experienced. If the patients who were given placebo first did not respond to the placebo, the addition of naloxone did not change patients' pain. This supports the hypothesis that endogenous opioids may be involved in the placebo analgesia response. To read the whole study please visit the additional resources page on this website to see the full referencing information.
The review article by Benedetti et al also mentions other mechanisms proposed regarding the physiology of placebo analgesia. They discuss mechanisms involving non-opioid mediators and cholecystokinin. In terms of non-opioid mediators, a study by Amanzio and Benedetti in 1999 showed that patients who underwent conditioning (see our theories page for more information on conditioning) with the drug Ketorolac experienced a placebo response that was non responsive to naloxone, meaning that the addition of naloxone after giving a placebo that produced a response, did not cause more pain in the patient. Therefore, other pathways besides the endogenous opioid pathway mentioned by Levine et al must be present in effects experienced through administration of placebo analgesia. Cholecystokinin (CCK) has also been proposed to be involved in the analgesia response experienced by patients given placebo. CCK exhibits the opposite action of opioids. In one study, when proglumide, a drug which blocks CCK was given, the relief of pain experienced by placebo was enhanced, thereby indicating CCK may also have a role in analgesia experienced through adminstration of a placebo. See the green box in the diagram above for more on these mechanisms.
Dopamine Release and Placebos
The use of placebos have also been implicated in Parkinson's Disease patients because of their ability to cause a release in dopamine in some patients. One study by de la Fuente-Fernandez et al used [11C] raclopride positive emission tomography scans (PET scans) to estimate dopamine release endogenously and activity in the nigrostriatal dopaminergic system. Patients were blinded and received a placebo or apomorphine, which is a dopamine agonist. It is important to note that dopamine competes with the raclopride for binding to D2 and D3 (dopamine 2 and 3) receptors. The results of this study showed that patients who were administered placebo showed increased endogenous dopamine release, exhibited by a decline in raclopride binding. This is indicative of dopamine release in the body.
The use of placebos have also been implicated in Parkinson's Disease patients because of their ability to cause a release in dopamine in some patients. One study by de la Fuente-Fernandez et al used [11C] raclopride positive emission tomography scans (PET scans) to estimate dopamine release endogenously and activity in the nigrostriatal dopaminergic system. Patients were blinded and received a placebo or apomorphine, which is a dopamine agonist. It is important to note that dopamine competes with the raclopride for binding to D2 and D3 (dopamine 2 and 3) receptors. The results of this study showed that patients who were administered placebo showed increased endogenous dopamine release, exhibited by a decline in raclopride binding. This is indicative of dopamine release in the body.
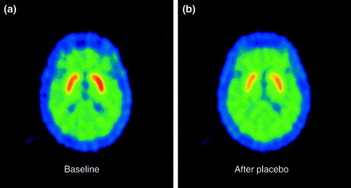
This figure is from another paper by de la Fuente-Ferndandez and Stoessl showing an example of dopamine release in response to placebo in Parkinson's Disease patients:
"[11C]raclopride (RAC)–PET scans of a patient with Parkinson's disease at open baseline (a) and after placebo administration (i.e. saline injected; b). The placebo-induced decrease in striatal radioactivity (indicated by the less intense red colour) is thought to reflect an increase in the synaptic level of dopamine, which inhibits RAC from binding to dopamine D2 receptor sites."
"[11C]raclopride (RAC)–PET scans of a patient with Parkinson's disease at open baseline (a) and after placebo administration (i.e. saline injected; b). The placebo-induced decrease in striatal radioactivity (indicated by the less intense red colour) is thought to reflect an increase in the synaptic level of dopamine, which inhibits RAC from binding to dopamine D2 receptor sites."
References:
1. Benedetti F, Mayber HS, Wager TD, Stohler CS, Zubieta JK. Neurobiological Mechanisms of the Placebo Effect. J Neurosci. 2005;25(45):10390-402.
2. Conrad Stopper M. Endorphins: Natural Pain and Stress Fighters. MedicineNet.com. http://www.medicinenet.com/script/main/art.asp?articlekey=55001. Updated March 25, 2007. Accessed May 28, 2013.
3. Levine JD, Gordon NC, Fields HL. The mechanism of placebo analgesia. Lancet. 1978;2(8091):654-7.
4. Amanzio M, Benedetti F. Neuropharmacological dissection of placebo analgesia: expectation activated opioid systems versus conditioning-activated specific subsystems. J Neurosci. 1999;19(1):484-94.
5. Oken BS. Placebo effects: clinical aspects and neurobiology. Brain. 2008; 131:2812-2823.
6. de la Fuente-Fernandez R, Ruth TJ, Sossi V, Schulzer M, Caine DB, Stoessl AJ. Expectation and Dopamine Release: Mechanism of the Placebo Effect in Parkinson's Disease. Science. 2001;293(5532):1164-6.7.
7. Apopmorphine. LexiComp. http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/6373. Updated 2013. Accessed May 29, 2013.
8. de la Fuente-Fernandez, Stoessl AJ. The placebo effect in Parkinson's Disease. Trends Neurosci. 2002;25(6):302-6.
Images courtesy of:
http://www.nature.com/nrn/journal/v6/n7/fig_tab/nrn1705_F2.html
http://www.sciencedirect.com/science/article/pii/S0166223602021811
http://www.clearmindcenter.com/the-neuro-map/
1. Benedetti F, Mayber HS, Wager TD, Stohler CS, Zubieta JK. Neurobiological Mechanisms of the Placebo Effect. J Neurosci. 2005;25(45):10390-402.
2. Conrad Stopper M. Endorphins: Natural Pain and Stress Fighters. MedicineNet.com. http://www.medicinenet.com/script/main/art.asp?articlekey=55001. Updated March 25, 2007. Accessed May 28, 2013.
3. Levine JD, Gordon NC, Fields HL. The mechanism of placebo analgesia. Lancet. 1978;2(8091):654-7.
4. Amanzio M, Benedetti F. Neuropharmacological dissection of placebo analgesia: expectation activated opioid systems versus conditioning-activated specific subsystems. J Neurosci. 1999;19(1):484-94.
5. Oken BS. Placebo effects: clinical aspects and neurobiology. Brain. 2008; 131:2812-2823.
6. de la Fuente-Fernandez R, Ruth TJ, Sossi V, Schulzer M, Caine DB, Stoessl AJ. Expectation and Dopamine Release: Mechanism of the Placebo Effect in Parkinson's Disease. Science. 2001;293(5532):1164-6.7.
7. Apopmorphine. LexiComp. http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/6373. Updated 2013. Accessed May 29, 2013.
8. de la Fuente-Fernandez, Stoessl AJ. The placebo effect in Parkinson's Disease. Trends Neurosci. 2002;25(6):302-6.
Images courtesy of:
http://www.nature.com/nrn/journal/v6/n7/fig_tab/nrn1705_F2.html
http://www.sciencedirect.com/science/article/pii/S0166223602021811
http://www.clearmindcenter.com/the-neuro-map/
